Most people get through their lives never knowing what a hiatus hernia is — until the burning starts. That familiar crawl of acid up the throat. The pressure behind the sternum that almost feels cardiac but isn’t. The meals that end in discomfort rather than satisfaction. And then, at some point, someone mentions the words hiatus hernia, and suddenly a whole picture starts to form.It’s more common than most people realize. It doesn’t always need surgery. But it does need attention. Ignoring persistent acid reflux in Hisar and surrounding areas — where spicy, hearty food is part of daily life — isn’t really a strategy. It just delays the conversation.
What Is a Hiatus Hernia, Actually
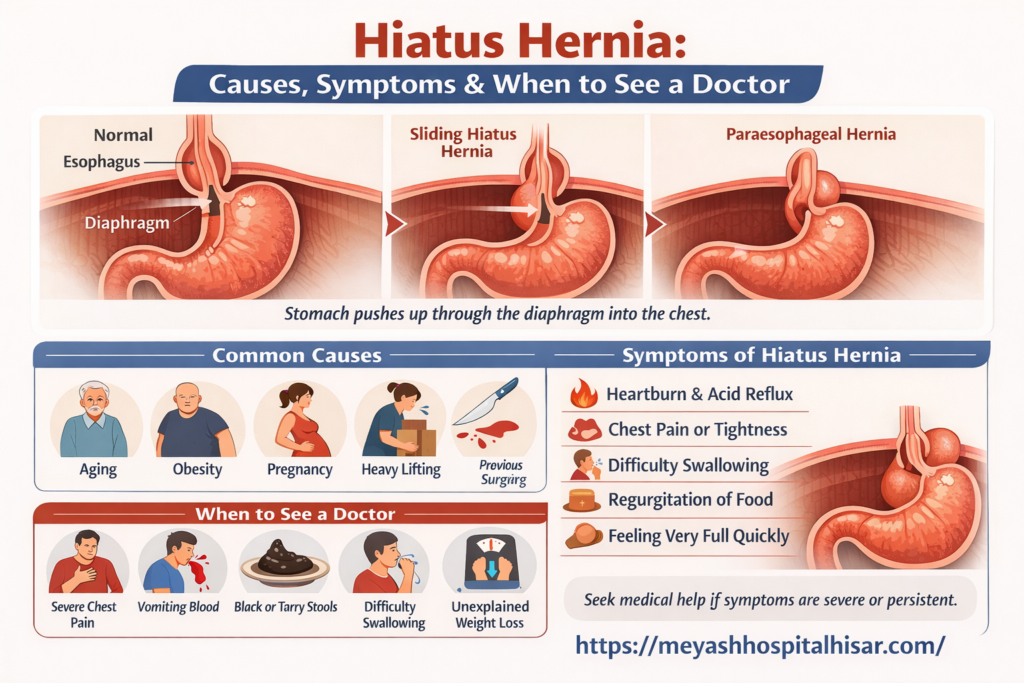
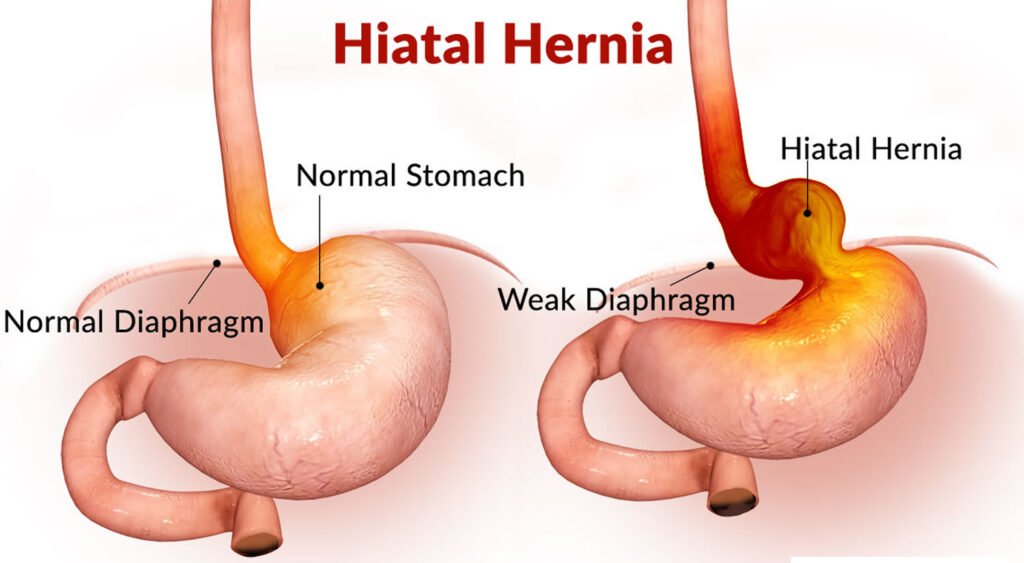
The diaphragm is the muscular sheet separating your chest cavity from your abdomen. There’s a small opening in it — called the hiatus — through which the esophagus passes down to connect to the stomach. In a hiatus hernia, part of the stomach pushes up through that opening into the chest cavity.
It sounds alarming. For most people, it’s a slow, quiet thing. The stomach nudges up a little. The valve between the esophagus and stomach — the lower esophageal sphincter — doesn’t work as well as it should. Acid that should stay down starts drifting up. That’s the basic mechanism.
Types Worth Knowing About
There are two main types and understanding the difference matters for what treatment looks like.
• Sliding hiatus hernia — the most common type. The junction between the esophagus and stomach slides up through the hiatus. This comes and goes with position and pressure. Usually causes reflux symptoms.
• Paraesophageal hernia — rarer and more concerning. Part of the stomach rolls up beside the esophagus. Can cause complications like obstruction or reduced blood supply to the herniated stomach. May require surgery even without obvious symptoms.
Most people have the sliding type. Most of them can be managed without surgery. But both types deserve proper diagnosis — you can’t tell from symptoms alone.
What Causes a Hiatus Hernia
There’s rarely a single cause. It’s usually accumulation. The diaphragm weakens with age. Repeated pressure events stretch the hiatus gradually.
• Age — the diaphragmatic tissue naturally loses elasticity over time. Hiatus hernias are more common in people over 50.
• Obesity — increased abdominal pressure pushes upward chronically. This is one of the most significant risk factors for both the hernia and its symptoms.
• Pregnancy — similar mechanism. The growing uterus pushes up on the stomach and diaphragm.
• Heavy lifting and straining — sudden pressure events, repeated over time. This includes chronic constipation too.
• Previous esophageal surgery or injury.
• Congenital factors — some people are simply born with a larger hiatal opening.
Lifestyle matters here but it’s not purely lifestyle. Some people who do everything right still develop this. Genetics plays a role that doesn’t get enough acknowledgment.
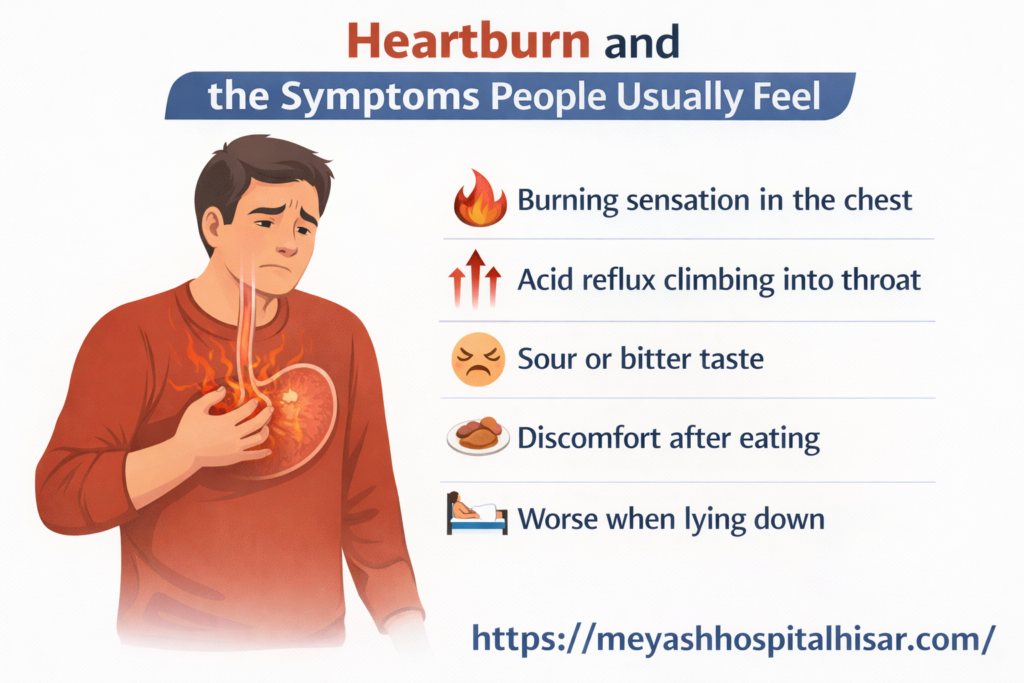
Heartburn and the Symptoms People Usually Feel
The classic presentation is heartburn. That burning sensation in the chest, usually after meals, often worse when lying down or bending forward. Acid reflux that climbs into the throat. A sour or bitter taste.
But hiatal hernia pain can present in ways that get misread. Chest tightness that gets investigated as a cardiac issue. Difficulty swallowing. Feeling full very quickly. Regurgitation without the burning sensation. In some people, there’s an irritating chronic cough — acid reaching the throat and airways causes a reflex cough that puzzles both patient and GP for months before the connection gets made.
Symptoms that feel more urgent. Not your average heartburn pattern.
• Severe chest or upper abdominal pain
• Vomiting blood or passing black stools
• Difficulty swallowing that is progressive or sudden
• Feeling of food being stuck
• Unexplained weight loss
These deserve prompt evaluation. Not next week. Soon.
When to Actually See a Doctor
The threshold question. A lot of people manage mild reflux with antacids from the pharmacy for years and never get a formal diagnosis. That works up to a point. But there are moments when a visit to a specialist is the right move.
If you’re taking antacids more than twice a week regularly, that’s a signal. If your symptoms have changed — gotten more frequent, more severe, or started waking you at night — that’s a signal. If you’re noticing difficulty swallowing or any of the alarm symptoms listed above, that’s not a signal. That’s a requirement.
For those experiencing persistent acid reflux in Hisar, seeing a gastroenterologist or a surgeon who specializes in upper GI conditions makes sense. Chronic uncontrolled acid reflux — regardless of the underlying cause — can over years lead to Barrett’s esophagus, a precancerous condition. Early diagnosis and management matters.
How It Gets Diagnosed
An upper GI endoscopy is the most definitive test. A camera passes through the mouth, down the esophagus, into the stomach. The doctor can see the hernia directly, assess the valve function, and look for any damage to the esophageal lining.
A barium swallow study — swallowing a contrast liquid and watching it on X-ray — is another method, especially for paraesophageal hernias. CT scanning is sometimes used. The choice depends on what the doctor suspects and what they need to see clearly.
Treatment: Not Always Surgery
Most hiatus hernias are managed without surgery. Lifestyle changes plus medication, for many people, achieves adequate control.
Losing weight if overweight. Smaller, more frequent meals. Avoiding lying down within 2-3 hours of eating. Elevating the head of the bed. Reducing trigger foods — fatty meals, citrus, tomato-based foods, coffee, alcohol, spicy food (challenging advice in Haryana, but relevant nonetheless). Stopping smoking.
Medications — proton pump inhibitors primarily — reduce acid production. H2 blockers are another class. These don’t fix the mechanical problem but they control the chemical consequences well enough for many people.
Surgery comes into the picture when symptoms aren’t controlled despite adequate medication and lifestyle changes, when the hernia is large or paraesophageal and at risk of complications, or when a patient wants a long-term solution without lifelong medication. The Nissen fundoplication — wrapping the upper stomach around the esophagus to reinforce the valve — is the most common surgical approach, and it’s done laparoscopically in most cases today.
Conclusion
Hiatus hernia is not a dramatic diagnosis but it deserves serious attention. Persistent heartburn, hiatal hernia pain, and reflux that disrupts sleep or diet aren’t just inconveniences. They’re the body flagging that something mechanical needs addressing. Whether that means lifestyle adjustment, medication, or surgery depends on the individual case. But the first step is always the same: stop guessing and get properly evaluated.
Frequently Asked Questions
1. Can a hiatus hernia go away on its own?
Not typically. The structural change to the diaphragm doesn’t reverse spontaneously. Symptoms can improve significantly with lifestyle and medication, but the hernia itself remains present.
2. Is heartburn always caused by a hiatus hernia?
No. Heartburn has many causes — poor diet, obesity, pregnancy, certain medications, or simply a weak lower esophageal sphincter without any hernia. A hiatus hernia Surgery is a frequent contributor but not the only explanation.
3. Is hiatus hernia dangerous?
The sliding type is usually not dangerous but can affect quality of life significantly. Paraesophageal hernias carry more risk of serious complications including obstruction or strangulation, which is why they’re often repaired surgically even when minimally symptomatic.
4. Can I eat normally with a hiatus hernia?
Many people do. It usually involves learning which foods trigger symptoms and moderating those. Smaller meals, slower eating, and not lying down immediately after eating help considerably.
5. How do I know if my chest pain is from a hiatus hernia or my heart?
You can’t know without evaluation. Cardiac causes must be ruled out first. If chest pain is new, severe, comes with shortness of breath, arm pain, or sweating, go to the emergency department. Once cardiac causes are excluded, gastroesophageal causes can be explored properly.