Most people who have a hiatus hernia don’t know it. They know the burning. The belching after meals. The uncomfortable feeling of food sitting wrong, of waking at 3am with acid climbing up the throat. They’ve blamed spicy food, late dinners, stress. They’ve taken antacids for years.
And then someone finally does a scope and says: you have a hiatal hernia.
Suddenly there’s a name for something that’s been happening for a long time. And suddenly there are questions. What is it, exactly? Will I need surgery? Is this serious? Why does it feel worse when I bend down or lie flat?
This post is for that moment. For people in Hisar and around who are sitting with a new diagnosis or a long-suspected condition and trying to understand what’s happening inside their own body.
What Is a Hiatus Hernia — Actually
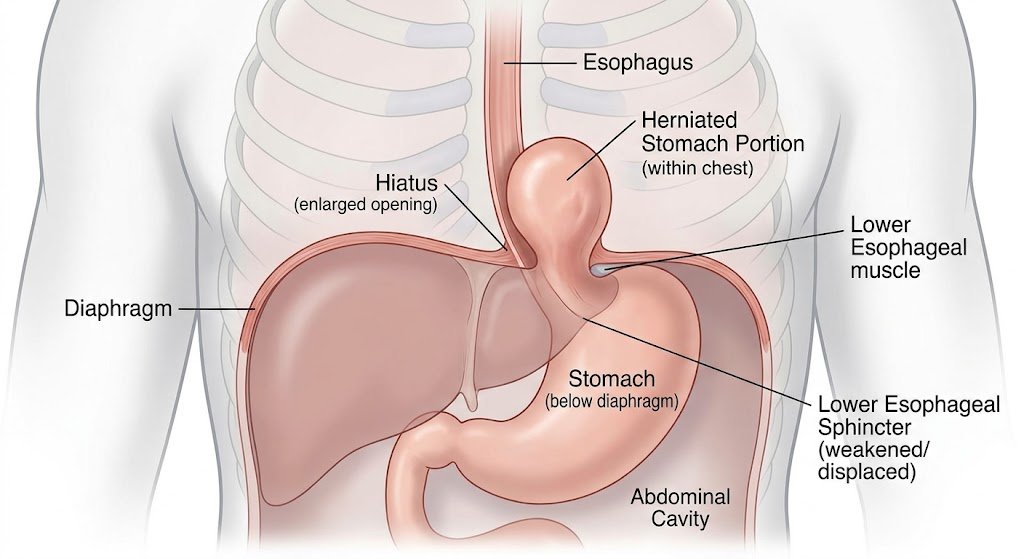
The hiatus is a small opening in your diaphragm — the large, dome-shaped muscle that separates your chest cavity from your abdomen. The oesophagus passes through this opening on its way to the stomach. In a hiatus hernia (also written hiatal hernia), the stomach pushes up through this opening into the chest cavity. Partially, or sometimes substantially.
It’s not as dramatic as it sounds. The stomach isn’t bursting through anything. It’s more like a gradual shift — the opening widens a little, the stomach slides up. But the consequences — particularly for acid reflux — can significantly affect daily life.
There are two main types:
• Sliding hiatal hernia — the most common type, where the stomach and lower oesophagus slide up into the chest, particularly when lying down or bending. This accounts for about 95% of all hiatal hernias
• Para-oesophageal hiatal hernia — rarer and more serious, where part of the stomach pushes through alongside the oesophagus. This type carries a higher risk of complications and is more likely to need surgery
Symptoms of Hiatus Hernia — The Ones People Actually Experience
The symptom list in medical texts can feel removed from what it actually feels like to live with a hiatal hernia. So here’s a more honest version:
• Persistent heartburn — not occasional, but often daily, particularly after meals, when lying down, or after bending over
• Acid reflux or GERD — stomach acid coming up into the throat, sometimes tasting sour or burning the back of the throat
• Regurgitation — food or liquid coming back up, especially when lying down
• Difficulty swallowing — a feeling of food getting stuck, particularly with solid foods
• Chest pain — which can mimic heart-related pain and understandably causes a lot of anxiety
• Belching and bloating — often worse after eating or drinking carbonated drinks
• Shortness of breath — in larger hernias, stomach pressing into the chest can compress lung space slightly
• Feeling full quickly — even small meals feel heavy or uncomfortable
Not everyone has all of these. Some people with a small hiatus hernia have almost no symptoms. Others with a moderate hernia are significantly affected. Symptom severity doesn’t always match hernia size.
Causes and Risk Factors — Why Does This Happen
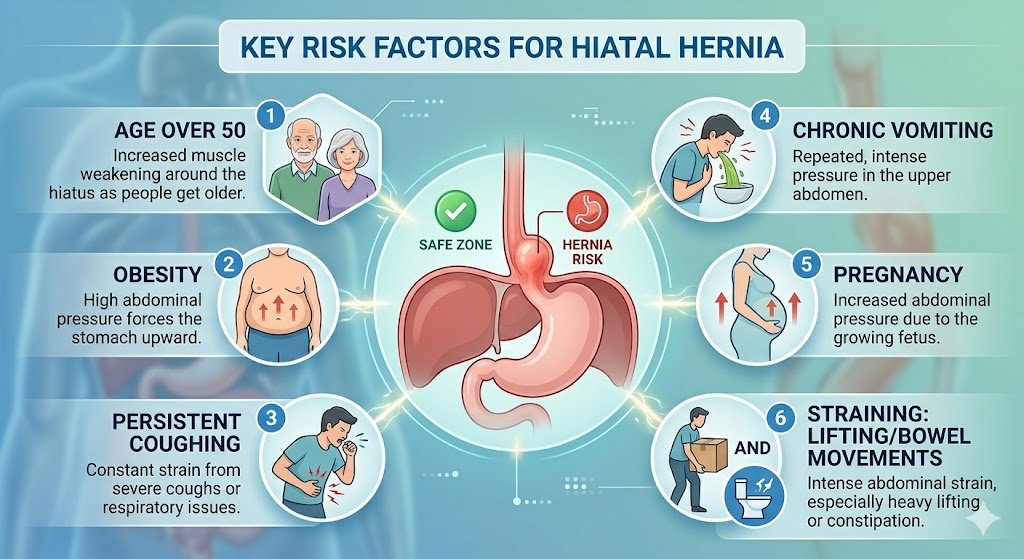
The honest answer is that for most people, there isn’t one clear cause. It’s usually a combination of factors over time:
• Age — the hiatal opening naturally weakens and widens with age; hiatal hernias are more common after 50
• Obesity — excess abdominal pressure pushes organs upward; this is one of the most significant modifiable risk factors
• Chronic coughing or straining — long-term cough from smoking or chest conditions, chronic constipation, or heavy lifting that increases abdominal pressure
• Pregnancy — increased pressure during pregnancy can contribute
• Previous trauma — injury to the diaphragm area
• Congenital factors — some people are born with a larger hiatal opening
In Hisar and across north India, dietary patterns — high intake of spicy food, late heavy dinners, excessive tea and chai — don’t cause hiatus hernia directly, but they significantly worsen symptoms once the hernia is present.
Diagnosis — How Is Hiatus Hernia Detected
A hiatal hernia is usually found in one of these ways:
• Upper endoscopy (gastroscopy) — a camera passed through the mouth into the oesophagus and stomach; the most accurate way to see a hiatal hernia and assess its size and any associated inflammation
• Barium swallow X-ray — the patient swallows barium liquid which shows up on X-ray, outlining the oesophagus and stomach
• CT scan — used for larger or more complex hernias, particularly para-oesophageal types
If you’re in Hisar and have persistent reflux symptoms that don’t respond well to medication, asking your doctor specifically about an endoscopy to rule out hiatus hernia is reasonable and worth doing.
Read More – Hiatus Hernia: Causes, Symptoms and When to Visit a Doctor
Treatment Options for Hiatus Hernia in Hisar
Treatment depends on the size of the hernia, the severity of symptoms, and whether there are complications. Not every hiatal hernia needs surgery.
Lifestyle Changes — The First Line
For small sliding hiatus hernias with manageable symptoms, lifestyle changes make a genuine difference:
• Eating smaller, more frequent meals rather than large ones
• Not lying down for at least 2 to 3 hours after eating
• Elevating the head of the bed by 15 to 20 cm — not just using extra pillows, which can make it worse
• Weight loss — even modest weight reduction significantly reduces abdominal pressure and symptom severity
• Avoiding trigger foods: spicy food, citrus, chocolate, coffee, alcohol, carbonated drinks
• Quitting smoking — smoking weakens the lower oesophageal sphincter
Medication for Hiatus Hernia
Medications don’t fix the hernia but they manage the acid that causes the most symptoms:
• Proton pump inhibitors (PPIs) — reduce acid production significantly; commonly prescribed, often long-term
• H2 blockers — less potent acid reducers, used for milder symptoms
• Antacids — provide quick relief but don’t address the underlying acid production
Long-term PPI use is common for hiatal hernia management but comes with its own considerations — potential effects on bone density and gut microbiome over years. This is a conversation worth having with your doctor if you’ve been on PPIs for a long time.
Surgery for Hiatus Hernia — When Is It Needed
Surgery is not the automatic answer, but it becomes the right answer when:
• Symptoms are severe and significantly affecting quality of life despite medication
• The hernia is large, particularly a para-oesophageal type with complications
• There is oesophageal damage — Barrett’s oesophagus or significant erosion
• The patient prefers a permanent solution over lifelong medication
• There is risk of strangulation in para-oesophageal hernias
The standard surgical procedure for hiatus hernia is called Nissen fundoplication — where the upper part of the stomach is wrapped around the lower oesophagus to strengthen the valve and prevent acid reflux. In Hisar, this is now performed laparoscopically in appropriate patients — meaning small incisions, shorter hospital stay, and faster recovery compared to open surgery.
Hiatal Hernia Surgery in Hisar — What to Expect
Laparoscopic hiatus hernia repair typically involves a one to two night hospital stay. Most patients experience significant relief from reflux symptoms after surgery. Recovery to light activity takes about one to two weeks, and full recovery is usually complete by four to six weeks.
It’s not a perfect solution — a small percentage of patients experience recurrence or new symptoms after surgery. The discussion with your surgeon in Hisar should include realistic expectations about what surgery can and cannot fix.
Conclusion
A hiatus hernia is a common condition that sits somewhere between lifestyle inconvenience and genuine medical problem, depending on its size and your symptoms. The good news is that most people can manage it well with a combination of lifestyle adjustments and medication. The further good news is that when surgery is needed, laparoscopic hiatal hernia repair in Hisar has become a safe, effective option with a manageable recovery.
If you’ve had unexplained reflux, difficulty swallowing, or chronic heartburn, get it investigated. A scope and a proper diagnosis is worth far more than years of guessing.
Frequently Asked Questions
1. Can a hiatus hernia go away on its own?
No. Once a hiatus hernia has formed, it doesn’t spontaneously resolve. However, symptoms can be well managed and in some cases significantly reduced through lifestyle changes and medication without needing surgery. You also need to maintain proper hiatus hernia diet to recover better and get fit as well.
2. Is hiatus hernia the same as GERD?
Not exactly, but they’re closely linked. Hiatal hernia is a structural condition — the stomach pushing through the diaphragm. GERD is the reflux of stomach acid. A hiatus hernia often contributes to or worsens GERD, but GERD can occur without a hiatal hernia too.
3. What foods should I avoid with a hiatus hernia?
Spicy foods, citrus fruits, chocolate, coffee, alcohol, carbonated drinks, and fatty or fried foods tend to worsen symptoms. Late heavy meals are particularly problematic. These don’t cause the hernia but they significantly aggravate it.
4. Is laparoscopic surgery for hiatus hernia available in Hisar?
Yes. Laparoscopic hiatus hernia repair is available in Hisar at facilities with trained laparoscopic surgeons. The procedure involves small incisions, shorter hospital stay, and faster recovery compared to open surgery.
5. Will I need to take medication forever if I don’t have surgery?
For significant hiatal hernia with ongoing symptoms, many patients do require long-term medication, particularly PPIs. The decision about continuing medication versus considering surgery is worth revisiting periodically with your doctor, especially if you’ve been on PPIs for several years.